Scoliosis
Story by Cheri Woodsmall
June is Scoliosis Awareness Month. Scoliosis, by definition, is an abnormal lateral curvature of the spine. It is most often diagnosed in childhood or early adolescence. The spine’s normal curves occur at the cervical, thoracic, and lumbar regions in the so-called “sagittal” plane. These natural curves position the head over the pelvis and work as shock absorbers to distribute mechanical stress during movement. Scoliosis is often defined as spinal curvature in the “coronal” (frontal) plane. While the degree of curvature is measured on the coronal plane, scoliosis is a more complex, three-dimensional problem which involves the following planes:
- CORONAL PLANE: A vertical plane from head to foot and parallel to the shoulders, dividing the body into anterior (front) and posterior (back) sections.
- SAGITTAL PLANE: Divides the body into right and left halves.
- AXIAL PLANE: Parallel to the plane of the ground and at right angles to the coronal and sagittal planes.
According to the National Scoliosis Foundation, Scoliosis affects 2-3 percent of the population, or an estimated six to nine million people in the United States. Scoliosis can develop in infancy or early childhood. However, the primary age of onset for scoliosis is 10-15 years old, occurring equally among both genders. Females are eight times more likely to progress to a curve magnitude that requires treatment. Every year, scoliosis patients make more than 600,000 visits to private physician offices, an estimated 30,000 children are fitted with a brace and 38,000 patients undergo spinal fusion surgery.
WHAT CAUSES SCOLIOSIS
Scoliosis can be classified by etiology: idiopathic, congenital, or neuromuscular.
Idiopathic scoliosis is the diagnosis when all other causes are excluded and comprises about 80 percent of all cases. Adolescent idiopathic scoliosis is the most common type of scoliosis and is usually diagnosed during puberty. Roughly 3 million new cases of the condition are diagnosed in the United States each year, with most of them identified as idiopathic scoliosis — a type of scoliosis that presents in children between 10 to 12 years old.
Congenital scoliosis results from embryological malformation of one or more vertebrae and may occur in any location of the spine. The vertebral abnormalities cause curvature and other deformities of the spine because one area of the spinal column lengthens at a slower rate than the rest. The geometry and location of the abnormalities determine the rate at which the scoliosis progresses in magnitude as the child grows. Because these abnormalities are present at birth, congenital scoliosis is usually detected at a younger age than idiopathic scoliosis.
Neuromuscular scoliosis encompasses scoliosis that is secondary to neurological or muscular diseases. This includes scoliosis associated with cerebral palsy, spinal cord trauma, muscular dystrophy, spinal muscular atrophy, and spina bifida. This type of scoliosis generally progresses more rapidly than idiopathic scoliosis and often requires surgical treatment.
WHAT ARE THE SIGNS AND SYMPTOMS?
If you have scoliosis, you might lean a little when you stand.
You could also have:
- A visible curve in your back
- Shoulders, a waist, or hips that look uneven
- One shoulder blade that looks bigger
- Head is not centered above the pelvis
- Ribs that stick out farther on one side of your body than the other
In addition to visible symptoms, scoliosis may lead to:
- Low back pain
- Back stiffness
- Pain and numbness in your legs (from pinched nerves)
- Fatigue due to muscle strain
THE DIAGNOSIS
To check for scoliosis, during a physical exam, your doctor might first ask you to bend over from the waist so they can see if your spine looks curved. Pediatricians often do this kind of exam on children.
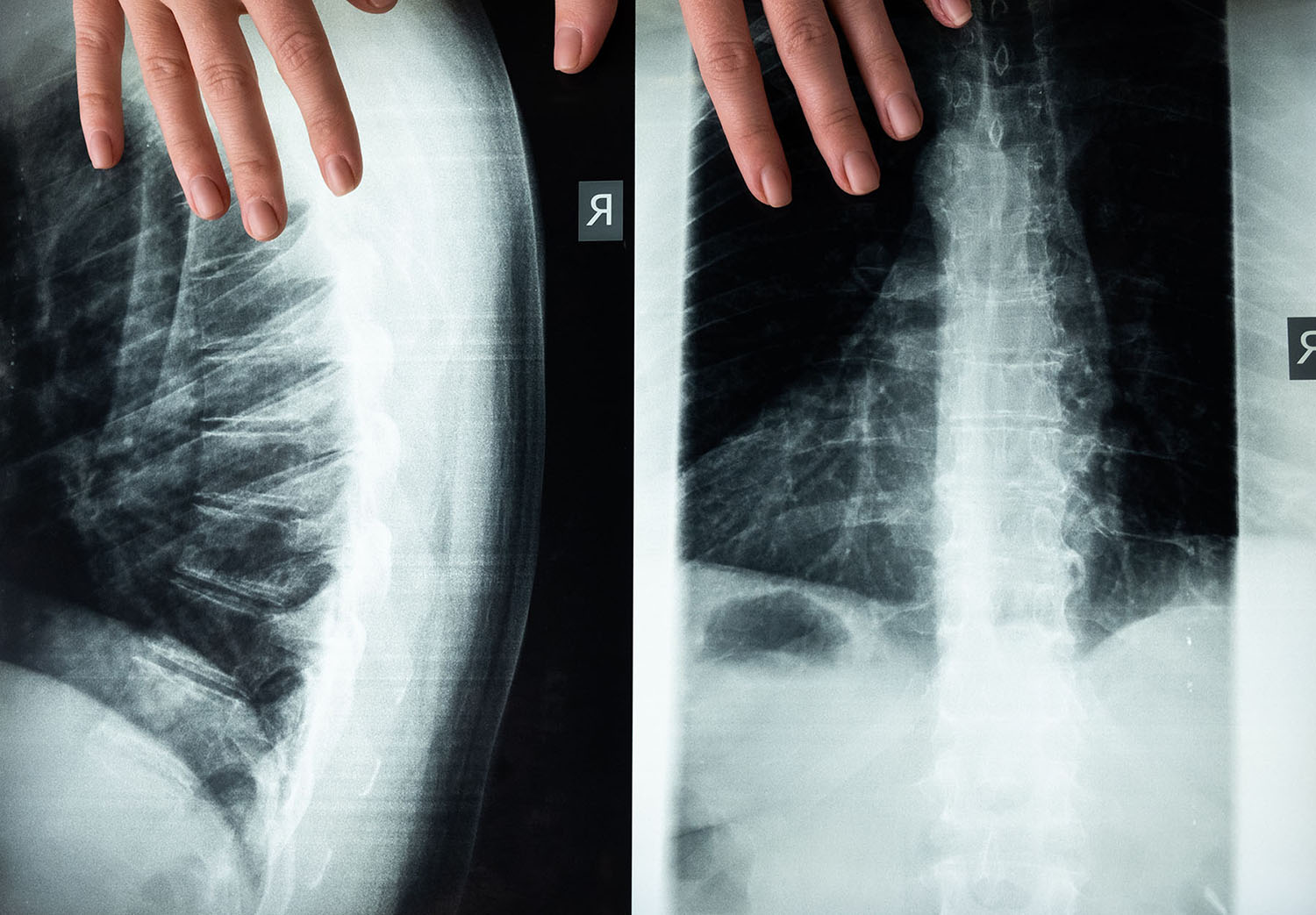
If your back looks curved, they will likely do an X-ray to see whether it is scoliosis. Your doctor might also do an MRI to rule out things like a tumor that could cause your spine to curve. The curve is measured by the Cobb Method and is diagnosed in terms of severity by the number of degrees.
A standard exam that is sometimes used by pediatricians and in grade school screenings is called the Adam’s Forward Bend Test. During this test, the patient leans forward with his or her feet together and bends 90 degrees at the waist. From this angle, any asymmetry of the trunk or any abnormal spinal curvatures can easily be detected by the examiner. This is a simple initial screening test that can detect potential problems but cannot determine accurately the exact type or severity of the deformity. Radiographic tests are required for an accurate and positive diagnosis.
- X-ray: Application of radiation to produce a film or picture of a part of the body can show the structure of the vertebrae and the outline of the joints. X-rays of the spine are obtained to search for other potential causes of pain, i.e., infections, fractures, deformities, etc.
- Computed tomography scan (CT or CAT scan): A diagnostic image created after a computer reads X-rays; can show the shape and size of the spinal canal, its contents, and the structures around it. Particularly good at visualizing bony structures.
- Magnetic resonance imaging (MRI): A diagnostic test that produces three-dimensional images of body structures using powerful magnets and computer technology; can show the spinal cord, nerve roots and surrounding areas, as well as enlargement, degeneration, and deformities.

SCOLIOSIS IN CHILDREN
As a parent, the first thing you might do is blame yourself. It is not a parent’s fault if their child is diagnosed with scoliosis. Parents tend to ask what they could have done to prevent scoliosis, but scoliosis is a remarkably interesting disease because there is currently no known cause or prevention method.
It is also quite common for parents to ask if bad posture or heavy backpacks could have caused their child’s scoliosis. While these two things may be associated with other spine and back conditions, they do not cause scoliosis.
If your child is diagnosed with scoliosis, do not to be scared. Scoliosis is a very manageable condition when diagnosed early. For children who are still growing, an external torso brace can be used to prevent further worsening of scoliosis while the child grows. Even when wearing a brace, most children live normal lives and participate in the same activities as their peers.
If your child turns out to be among them, doctor’s will advise parents that while it may be a hard decision to make on behalf of your child, having surgery sooner rather than later is better. When done early, the surgery tends to be simpler, as less of the spine needs to be fused. Perhaps more importantly, is your child being in good overall health and having the support of his or her family during recovery. Parents should also work with their child’s school to determine a plan for the time the child will miss during recovery — usually one to two months.
SCOLIOSIS IN ADULTS
When scoliosis begins or is found after puberty, it is called “adult scoliosis” because the curve is discovered after complete skeletal growth.
Most adults with scoliosis can be divided into the following categories:
- Adult scoliosis patients who were surgically treated as adolescents.
- Adults who did not receive treatment when they were younger.
- Adults with a type of scoliosis called degenerative scoliosis.
Degenerative scoliosis occurs most frequently in the lumbar spine (lower back) and more commonly affects people aged 65 and older. It is often accompanied by spinal stenosis, or narrowing of the spinal canal, which pinches the spinal nerves and makes it difficult for them to function normally. Back pain associated with degenerative scoliosis usually begins gradually and is linked with activity. The curvature of the spine in this form of scoliosis is often relatively minor, so surgery may only be advised when conservative methods fail to alleviate pain associated with the condition.
TREATMENT
When there is a confirmed diagnosis of scoliosis, there are several issues to assess that can help determine treatment options:
- Spinal maturity – is the patient’s spine still growing and changing?
- Degree and extent of curvature – how severe is the curve and how does it affect the patient’s lifestyle?
- Location of curve – according to some experts, thoracic curves are more likely to progress than curves in other regions of the spine.
- Possibility of curve progression – patients who have large curves prior to their adolescent growth spurts are more likely to experience curve progression.
After these variables are assessed, the following treatment options may be recommended:
- Observation: Mild curves, like those found in 90% of scoliosis cases, typically don’t require treatment. Most cases of adult scoliosis can be managed non-operatively through regular observation by a doctor, over-the-counter pain medications, and core-strengthening exercises to strengthen your abdomen and back and to improve flexibility.
- Bracing: A scoliosis curve usually does not improve without surgery. However, studies have shown that wearing a back brace as prescribed can often prevent the progression of scoliosis. As such, wearing a brace can be an effective way to keep a scoliosis curve’s Cobb angle relatively small and manageable.
- Surgery: In children, the two primary goals of surgery are to stop the curve from progressing during adulthood and to diminish spinal deformity. Most experts would recommend surgery only when the spinal curve is greater than 40 degrees and there are signs of progression. This surgery can be done using an anterior approach (through the front) or a posterior approach (through the back) depending on the case.
Some adults who were treated as children may need revision surgery, if they were treated 20 to 30 years ago, before major advances in spinal surgery procedures were implemented.
In general, surgery in adults may be recommended when the spinal curve is greater than 50 degrees and the patient has nerve damage to their legs and/or is experiencing bowel or bladder symptoms. Adults with degenerative scoliosis and spinal stenosis may require decompression surgery with spinal fusion and a surgical approach from both the front and back.
HOW TO GET INVOLVED
1. Follow @ScoliosisResearchSociety on Facebook for information and events
2. Follow curvygirlsscoliosis.com a network of peer-led support groups that reduce the emotional impact of scoliosis by empowering girls through education, mutual support, and acceptance to become leaders, make healthy lifestyle choices, improve self-esteem while giving back to the Curvy Girls community.






